1.The Psychophysiological Unity of Sexual Response
In the clinical environment, sexual response must be evaluated as a unified psychophysiological event rather than a fragmented biological reflex. Physical responses are inextricably linked to a patient’s emotional state and mental filters; to treat one without the other is a fundamental diagnostic oversight. As practitioners, we must recognize that a healthy response is a total-body experience where physiological markers and psychological attitudes operate in a state of constant, mutual influence.
The core of this unity lies in the dual triggers of arousal: psychological and physical stimuli. These stimuli do not act in isolation but converge to create levels of tension experienced simultaneously across both somatic and emotional domains. When this tension culminates in orgasm, the resulting “feeling of well-being” serves as a critical clinical indicator. This subjective sense of satisfaction is the primary evidence of successful psychophysiological integration—it confirms that the mechanical release of tension (detumescence) has been harmonized with the patient’s emotional state. Without this internal sense of wellness, the achievement of physiological benchmarks remains an incomplete clinical outcome. This unity underscores that the mind effectively governs the physical mechanics of the response cycle.
- Psychological Determinants of Physical Outcomes
The practitioner’s role includes assessing the mental “filters” that either facilitate or inhibit the body’s innate sexual mechanics. While the physiological capacity for response may be intact, the mental state dictates whether that capacity is realized. We must view the mind as the primary modulator of the body’s autonomic sexual functions.
There are four specific psychological pillars that dictate these physical outcomes:
- Physical Health: The baseline somatic state of the patient.
- Psychosexual Development: The historical trajectory of the patient’s sexual identity and experiences.
- Psychological Attitudes Toward Sexuality: Internalized beliefs and moral frameworks regarding sex.
- Attitudes Toward the Sexual Partner: The specific emotional and relational dynamics within the partnership.
Positive attitudes across these pillars act as catalysts for physiological progression. Conversely, negative attitudes or “asexual stimuli”—such as a sudden loud noise or intrusive thoughts—can cause immediate physiological reversals, such as the precipitous loss of an erection. This illustrates the high sensitivity of the sexual system to psychological disruption. These mental states manifest physically through the two primary mechanisms of the sexual response: vasocongestion and myotonia.
- The Mechanics of Response: Vasocongestion and Myotonia
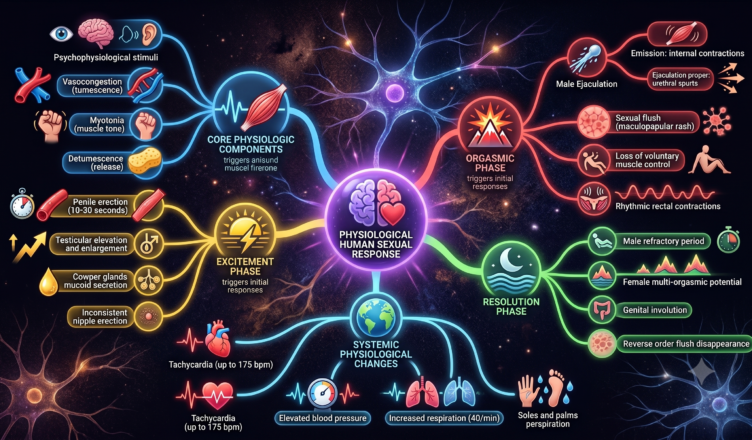
The foundational observations of Masters and Johnson provide the necessary framework for interpreting the body’s physical “language” during sexual activity. All observable physical changes in the sexual response cycle are driven by two core processes: vasocongestion (vascular engorgement) and myotonia (increased muscle tone).
Vasocongestion involves the concentration of blood in specific erectile tissues, leading to tumescence, while myotonia refers to both voluntary and involuntary increases in muscle tension. Clinically, the focus must be placed on the accumulation of these forces and their subsequent release during orgasm, known as detumescence. The “release” phase is as significant as the “build-up”; a failure to achieve a complete release of vascular activity and muscle tone can result in residual physical tension and psychological dissatisfaction. These mechanics follow a structured progression through specific chronological phases.
- Phase-Specific Physiological Analysis
Practitioners must meticulously track the progression from Excitement to Resolution to identify where a patient’s response cycle may be fluctuating, stalling, or deviating from healthy norms.
Excitement and Heightened Excitement Phases
The general Excitement Phase can span from several minutes to several hours. Penile erection typically occurs within 10–30 seconds via vasocongestion. However, we must distinguish this from the Heightened Excitement Phase—the period immediately preceding orgasm lasting only 30 seconds to 3 minutes.
- Anatomical Markers: During Heightened Excitement, the testes increase in size by 50% and flatten against the perineum; this flattening is the specific diagnostic signal of impending ejaculation.
- Secretions: Notably, the Cowper glands secrete 2–3 drops of mucoid fluid. It is vital for patient education to note that this fluid contains viable sperm, presenting a risk of pregnancy even prior to ejaculation.
- Autonomic Indicators: The “sexual flush”—an inconsistent maculopapular rash originating on the abdomen and spreading to the chest and face—may appear. Clinicians should view the absence of this flush as a normal variation rather than a pathology.
Orgasmic Phase
This phase is brief (3–15 seconds) and characterized by a total loss of voluntary muscular control.
- Myotonia: Involuntary semispastic contractions occur specifically in the facial, abdominal, and intercostal muscles.
- Rhythmic Precision: Male ejaculation occurs in two stages (emission and ejaculation proper). In both stages, contractions occur at precise 0.8-second intervals.
- Systemic Intensity: This phase involves extreme autonomic nervous system involvement. We observe Tachycardia (up to 175 beats/min), respiratory increases (up to 40 breaths/min), and significant blood pressure elevation (40–100 mm Hg systolic and 20–50 mm Hg diastolic increases).
Resolution Phase
Resolution involves the return to baseline over 10–15 minutes (or up to 24 hours if no orgasm occurred). The sexual flush disappears in reverse order of its appearance, and the scrotum and testes descend and return to baseline size within 5–30 minutes as vasocongestion is lost. This phase highlights the distinct recovery patterns between genders.
- Gender-Specific Dynamics and the Refractory Period
Effective counseling requires an understanding of the recovery patterns that differentiate the male and female experiences. The most significant physiological divergence is the male Refractory Period, a window following orgasm during which restimulation to further arousal is impossible. In contrast, women do not experience a refractory period and maintain the capacity for multiple, successive orgasms.
The male refractory period is highly dependent on age and situational novelty. Age significantly dictates the intensity and recovery of the system; for instance, an 18-year-old may experience an ejaculatory spurt of 12–20 inches, whereas a 70-year-old may experience only seepage. Managing patient expectations regarding these physiological changes is crucial for maintaining sexual confidence throughout the lifespan. These objective recovery patterns, however, must always be weighed against the patient’s internal experience.
- Subjectivity and the Synthesis of Satisfaction
While physiological markers—such as the 0.8-second contraction interval or the elevation of blood pressure—provide objective data, the practitioner’s ultimate priority must be the patient’s subjective satisfaction.
The sequence of sexual response is not strictly linear; phases frequently overlap and fluctuate. Consequently, the achievement of physiological benchmarks (like orgasm) does not inherently guarantee a successful clinical outcome. If a patient achieves orgasm but lacks the accompanying “feeling of well-being,” the practitioner must investigate the psychological pillars and filters that may be inhibiting satisfaction. Conversely, a patient may report high levels of satisfaction even if certain physiological markers, such as the sexual flush, are absent.
Ultimately, sexual health requires a holistic synthesis where the mind and body are treated as a single, interacting system. By prioritizing the patient’s perception of the experience alongside objective data, the clinician can facilitate a more profound and sustainable state of sexual health.
